
Rotator Cuff Tears: Frequently Asked Questions
-
1Rotator Cuff Tears: Frequently Asked Questions
Rotator Cuff Tears: Frequently Asked Questions
What is the rotator cuff and what does it do?
The rotator cuff is a group of four muscles that come together as tendons to form a «cuff» over the head of the humerus (upper arm bone). The four muscles—supraspinatus, infraspinatus, subscapularis and teres minor—originate from the scapula (shoulder blade). The rotator cuff tendons attach to the head of the humerus in special spots referred to as the greater and lesser tuberosities.
The rotator cuff helps to lift and rotate the arm and to stabilize the ball of the shoulder within the joint.
-
2What causes a rotator cuff tear and how would I know if I have one?
What causes a rotator cuff tear and how would I know if I have one?
A rotator cuff tear may result from an acute injury, such as a fall, or may be caused by normal age-related wear and tear with degeneration of the tendon.
Typically, you will feel pain in the front of your shoulder that radiates down the side of your arm. It may be present with overhead activities such as lifting or reaching. You may feel pain when you try to sleep on the affected side. You may note weakness of your arm and difficulty with routine activities such as combing your hair or reaching behind your back.
If the tear occurs with injury, you may experience acute pain, a snapping sensation, and immediate weakness of the arm
-
3If I have a painful rotator cuff and keep using it, will this cause further damage?
If I have a painful rotator cuff and keep using it, will this cause further damage?
A rotator cuff tear can extend or get larger over time. This can occur with repetitive use or a re-injury. It is common for patients with known rotator cuff disease to have acute pain and weakness following a minor injury. This likely represents extension of an existing tear.
If you know you have a rotator cuff tear, then worsening pain and decreasing strength may mean the tear is getting larger.
-
4When should I see a doctor for a rotator cuff tear?
When should I see a doctor for a rotator cuff tear?
If you have injured your shoulder or have chronic shoulder and arm pain, it is best to see your orthopaedic surgeon. He or she can then make a diagnosis and begin treatment. Your doctor may recommend a diagnostic imaging study such as a magnetic resonance imaging (MRI) scan or an ultrasound to confirm the diagnosis.
Early diagnosis and treatment of a rotator cuff tear may prevent symptoms such as loss of strength and loss of motion from setting in.
If your primary physician has already made the diagnosis, an orthopaedic surgeon can review both surgical and nonsurgical options and start treatment.
-
5Can a rotator cuff tear be healed or strengthened without surgery?
Can a rotator cuff tear be healed or strengthened without surgery?
Many rotator cuff tears can be treated nonsurgically. Anti-inflammatory medication, steroid injections, and physical therapy may all be of benefit in treating symptoms of a cuff tear. The goals of treatment are to relieve pain and restore strength to the involved shoulder.
Even though most tears cannot heal on their own, good function can often be achieved without surgery.
If, however, you are active and use your arm for overhead work or sports, then surgery is most often recommended because many tears will not heal without surgery.
-
6At what point does a rotator cuff tear require surgery to fix it?
At what point does a rotator cuff tear require surgery to fix it?
Surgery is recommended if you have persistent pain or weakness in your shoulder that does not improve with nonsurgical treatment. Frequently, patients who require surgery will report pain at night and difficulty using the arm for lifting and reaching. Many will report ongoing symptoms despite several months of medication and limited use of the arm.
Surgery is also indicated in active individuals who use the arm for overhead work or sports. Pitchers, swimmers, and tennis players are common examples.
-
7What options are available for surgical repair?
What options are available for surgical repair?
The type of repair performed is based on the findings at surgery. A partial tear may require only a trimming or smoothing procedure called a débridement. A full-thickness tear within the substance of the tendon can be repaired side to side. If the tendon is torn from its insertion on the humerus (the most common injury), it is repaired directly to bone.
Three techniques are used for rotator cuff repair: traditional open repair, mini-open repair, and arthroscopic repair.
Your orthopaedic surgeon can recommend which technique is best for you.
-
8How important is rehabilitation in the treatment of a rotator cuff tear?
How important is rehabilitation in the treatment of a rotator cuff tear?
Rehabilitation plays a critical role in both the nonsurgical and surgical treatment of a rotator cuff tear.
When a tear occurs, there is frequently atrophy of the muscles around the arm and loss of motion of the shoulder. An exercise or physical therapy program is necessary to regain strength and improve function in the shoulder.
Even though surgery repairs the defect in the tendon, the muscles around the arm remain weak, and a strong effort at rehabilitation is necessary for the procedure to succeed. Complete rehabilitation after surgery may take several months.
Your orthopaedic surgeon can prescribe an appropriate program based on your needs and the findings at surgery.
Shoulder Impingement/Rotator Cuff Tendinitis
-
1Shoulder Impingement
Shoulder Impingement/Rotator Cuff Tendinitis
One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great range of motion in your arm. Because so many different structures make up the shoulder, it is vulnerable to many different problems. The rotator cuff is a frequent source of pain in the shoulder.
-
2Anatomy
Anatomy
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
Your arm is kept in your shoulder socket by your rotator cuff. These muscles and tendons form a covering around the head of your upper arm bone and attach it to your shoulder blade.
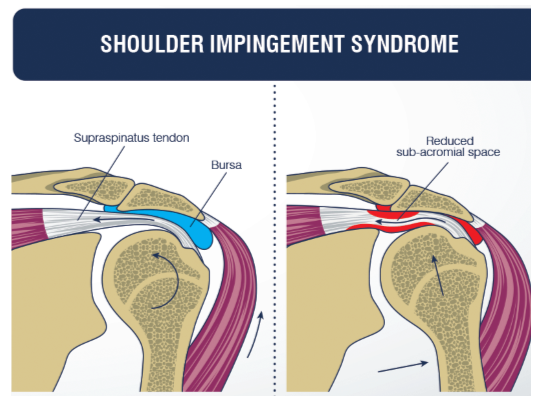
There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm.
-
3Description
Description
The rotator cuff is a common source of pain in the shoulder. Pain can be the result of:
- Tendinitis. The rotator cuff tendons can be irritated or damaged.
- Bursitis. The bursa can become inflamed and swell with more fluid causing pain.
- Impingement. When you raise your arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or «impinge» on) the tendon and the bursa, causing irritation and pain.
-
4Cause
Cause
Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible.
Pain may also develop as the result of a minor injury. Sometimes, it occurs with no apparent cause.
-
5Symptoms
Symptoms
Rotator cuff pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position.
Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage. These symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
- If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
-
6Doctor Examination
Doctor Examination
Medical History and Physical Examination
After discussing your symptoms and medical history, your doctor will examine your shoulder. He or she will check to see whether it is tender in any area or whether there is a deformity. To measure the range of motion of your shoulder, your doctor will have you move your arm in several different directions. He or she will also test your arm strength.Your doctor will check for other problems with your shoulder joint. He or she may also examine your neck to make sure that the pain is not coming from a «pinched nerve,» and to rule out other conditions, such as arthritis.
Imaging Tests
Other tests which may help your doctor confirm your diagnosis include:X-rays. Becauses x-rays do not show the soft tissues of your shoulder like the rotator cuff, plain x-rays of a shoulder with rotator cuff pain are usually normal or may show a small bone spur. A special x-ray view, called an «outlet view,» sometimes will show a small bone spur on the front edge of the acromion.
Magnetic resonance imaging (MRI) and ultrasound. These studies can create better images of soft tissues like the rotator cuff tendons. They can show fluid or inflammation in the bursa and rotator cuff. In some cases, partial tearing of the rotator cuff will be seen.
-
7Treatment
Treatment
The goal of treatment is to reduce pain and restore function. In planning your treatment, your doctor will consider your age, activity level, and general health.
Nonsurgical Treatment
In most cases, initial treatment is nonsurgical. Although nonsurgical treatment may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest. Your doctor may suggest rest and activity modification, such as avoiding overhead activities.
Non-steroidal anti-inflammatory medicines. Drugs like ibuprofen and naproxen reduce pain and swelling.
Physical therapy. A physical therapist will initially focus on restoring normal motion to your shoulder. Stretching exercises to improve range of motion are very helpful. If you have difficulty reaching behind your back, you may have developed tightness of the posterior capsule of the shoulder (capsule refers to the inner lining of the shoulder and posterior refers to the back of the shoulder). Specific stretching of the posterior capsule can be very effective in relieving pain in the shoulder.
Once your pain is improving, your therapist can start you on a strengthening program for the rotator cuff muscles.
Steroid injection. If rest, medications, and physical therapy do not relieve your pain, an injection of a local anesthetic and a cortisone preparation may be helpful. Cortisone is a very effective anti-inflammatory medicine. Injecting it into the bursa beneath the acromion can relieve pain.
Surgical Treatment
When nonsurgical treatment does not relieve pain, your doctor may recommend surgery.
The goal of surgery is to create more space for the rotator cuff. To do this, your doctor will remove the inflamed portion of the bursa. He or she may also perform an anterior acromioplasty, in which part of the acromion is removed. This is also known as a subacromial decompression. These procedures can be performed using either an arthroscopic or open technique.
Arthroscopic technique. In arthroscopy, thin surgical instruments are inserted into two or three small puncture wounds around your shoulder. Your doctor examines your shoulder through a fiberoptic scope connected to a television camera. He or she guides the small instruments using a video monitor, and removes bone and soft tissue. In most cases, the front edge of the acromion is removed along with some of the bursal tissue.
Your surgeon may also treat other conditions present in the shoulder at the time of surgery. These can include arthritis between the clavicle (collarbone) and the acromion (acromioclavicular arthritis), inflammation of the biceps tendon (biceps tendonitis), or a partial rotator cuff tear.
Open surgical technique. In open surgery, your doctor will make a small incision in the front of your shoulder. This allows your doctor to see the acromion and rotator cuff directly.
Rehabilitation. After surgery, your arm may be placed in a sling for a short period of time. This allows for early healing. As soon as your comfort allows, your doctor will remove the sling to begin exercise and use of the arm.
Your doctor will provide a rehabilitation program based on your needs and the findings at surgery. This will include exercises to regain range of motion of the shoulder and strength of the arm. It typically takes 2 to 4 months to achieve complete relief of pain, but it may take up to a year.
Shoulder Injuries in the Throwing Athlete
-
1Shoulder Injuries in the Throwing Athlete
Shoulder Injuries in the Throwing Athlete
Overhand throwing places extremely high stresses on the shoulder, specifically to the anatomy that keeps the shoulder stable. In throwing athletes, these high stresses are repeated many times and can lead to a wide range of overuse injuries.
Although throwing injuries in the shoulder most commonly occur in baseball pitchers, they can be seen in any athlete who participates in sports that require repetitive overhand motions, such as volleyball, tennis, and some track and field events.
-
2Anatomy
Anatomy
Your shoulder is a ball-and-socket joint made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. Surrounding the outside edge of the glenoid is a rim of strong, fibrous tissue called the labrum. The labrum helps to deepen the socket and stabilize the shoulder joint. It also serves as an attachment point for many of the ligaments of the shoulder, as well as one of the tendons from the biceps muscle in the arm.
Strong connective tissue, called the shoulder capsule, is the ligament system of the shoulder and keeps the head of the upper arm bone centered in the glenoid socket. This tissue covers the shoulder joint and attaches the upper end of the arm bone to the shoulder blade.
Your shoulder also relies on strong tendons and muscles to keep your shoulder stable. Some of these muscles are called the rotator cuff. The rotator cuff is made up of four muscles that come together as tendons to form a covering or cuff of tissue around the head of the humerus.
The biceps muscle in the upper arm has two tendons that attach it to the shoulder blade. The long head attaches to the top of the shoulder socket (glenoid). The short head attaches to a bump on the shoulder blade called the coracoid process. These attachments help to center the humeral head in the glenoid socket.
In addition to the ligaments and rotator cuff, muscles in the upper back play an important role in keeping the shoulder stable. These muscles include the trapezius, levator scapulae, rhomboids, and serratus anterior, and they are referred to as the scapular stabilizers. They control the scapula and clavicle bones — called the shoulder girdle — which functions as the foundation for the shoulder joint.
-
3Cause
Cause
When athletes throw repeatedly at high speed, significant stresses are placed on the anatomical structures that keep the humeral head centered in the glenoid socket.
Of the five phases that make up the pitching motion, the late cocking and follow-through phases place the greatest forces on the shoulder.
Late-cocking phase. In order to generate maximum pitch speed, the thrower must bring the arm and hand up and behind the body during the late cocking phase. This arm position of extreme external rotation helps the thrower put speed on the ball, however, it also forces the head of the humerus forward which places significant stress on the ligaments in the front of the shoulder. Over time, the ligaments loosen, resulting in greater external rotation and greater pitching speed, but less shoulder stability.
Follow-through phase. During acceleration, the arm rapidly rotates internally. Once the ball is released, follow-through begins and the ligaments and rotator cuff tendons at the back of the shoulder must handle significant stresses to decelerate the arm and control the humeral head.
When one structure — such as the ligament system — becomes weakened due to repetitive stresses, other structures must handle the overload. As a result, a wide range of shoulder injuries can occur in the throwing athlete.The rotator cuff and labrum are the shoulder structures most vulnerable to throwing injuries.
Common Throwing Injuries In the Shoulder
SLAP Tears (Superior Labrum Anterior to Posterior)
In a SLAP injury, the top (superior) part of the labrum is injured. This top area is also where the long head of the biceps tendon attaches to the labrum. A SLAP tear occurs both in front (anterior) and in back (posterior) of this attachment point.Typical symptoms are a catching or locking sensation, and pain with certain shoulder movements. Pain deep within the shoulder or with certain arm positions is also common.
Bicep Tendinitis and Tendon Tears
Repetitive throwing can inflame and irritate the upper biceps tendon. This is called biceps tendinitis. Pain in the front of the shoulder and weakness are common symptoms of biceps tendinitis.Occasionally, the damage to the tendon caused by tendinitis can result in a tear. A torn biceps tendon may cause a sudden, sharp pain in the upper arm. Some people will hear a popping or snapping noise when the tendon tears.
Rotator Cuff Tendinitis and Tears
When a muscle or tendon is overworked, it can become inflamed. The rotator cuff is frequently irritated in throwers, resulting in tendinitis.Early symptoms include pain that radiates from the front of the shoulder to the side of the arm. Pain may be present during throwing, other activities, and at rest. As the problem progresses, pain may occur at night, and the athlete may experience a loss of strength and motion.
Rotator cuff tears often begin by fraying. As the damage worsens, the tendon can tear. When one or more of the rotator cuff tendons is torn, the tendon no longer fully attaches to the head of the humerus. Most tears in throwing athletes occur in the supraspinatus tendon.
Problems with the rotator cuff often lead to shoulder bursitis. There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm. When the rotator cuff tendons are injured or damaged, this bursa can also become inflamed and painful.
Internal Impingement
During the cocking phase of an overhand throw, the rotator cuff tendons at the back of the shoulder can get pinched between the humeral head and the glenoid. This is called internal impingement and may result in a partial tearing of the rotator cuff tendon. Internal impingement may also damage the labrum, causing part of it to peel off from the glenoid.Internal impingement may be due to some looseness in the structures at the front of the joint, as well as tightness in the back of the shoulder.
Instability
Shoulder instability occurs when the head of the humerus slips out of the shoulder socket (dislocation). When the shoulder is loose and moves out of place repeatedly, it is called chronic shoulder instability.In throwers, instability develops gradually over years from repetitive throwing that stretches the ligaments and creates increased laxity (looseness). If the rotator cuff structures are not able to control the laxity, then the shoulder will slip slightly off-center (subluxation) during the throwing motion.
Pain and loss of throwing velocity will be the initial symptoms, rather than a sensation of the shoulder «slipping out of place.» Occasionally, the thrower may feel the arm «go dead.» A common term for instability many years ago was «dead arm syndrome.»
Glenohumeral Internal Rotation Deficit (GIRD)
As mentioned above, the extreme external rotation required to throw at high speeds typically causes the ligaments at the front of the shoulder to stretch and loosen. A natural and common result is that the soft tissues in the back of the shoulder tighten, leading to loss of internal rotation.This loss of internal rotation puts throwers at greater risk for labral and rotator cuff tears.
Scapular Rotation Dysfunction (SICK Scapula)
Proper movement and rotation of the scapula over the chest wall is important during the throwing motion. The scapula (shoulder blade) connects to only one other bone: the clavicle. As a result, the scapula relies on several muscles in the upper back to keep it in position to support healthy shoulder movement.
During throwing, repetitive use of scapular muscles creates changes in the muscles that affect the position of the scapula and increase the risk of shoulder injury.
Scapular rotation dysfunction is characterized by drooping of the affected shoulder. The most common symptom is pain at the front of the shoulder, near the collarbone.
In many throwing athletes with SICK scapula, the chest muscles tighten in response to changes in the upper back muscles. Lifting weights and chest strengthening exercises can aggravate this condition.
-
4Doctor Examination
Doctor Examination
Medical History and Physical Examination
The medical history portion of the initial doctor visit includes discussion about your general medical health, symptoms and when they first began, and the nature and frequency of athletic participationDuring the physicial examination, your doctor will check the range of motion, strength, and stability of your shoulder. He or she may perform specific tests by placing your arm in different positions to reproduce your symptoms.
The results of these tests help the doctor decide if additional testing or imaging of the shoulder is necessary.
Imaging Tests
Your doctor may order tests to confirm your diagnosis and identify any associated problems.X-rays. This imaging test creates clear pictures of dense structures, like bone. X-rays will show any problems within the bones of your shoulder, such as arthritis or fractures.
Magnetic resonance imaging (MRI). This imaging study shows better images of soft tissues. It may help your doctor identify injuries to the labrum, ligaments, and tendons surrounding your shoulder joint.
Computed tomography (CT) scan. This test combines x-rays with computer technology to produce a very detailed view of the bones in the shoulder area.
Ultrasound. Real time images of muscles, tendons, ligaments, joints, and soft tissues can be produced using ultrasound. This test is typically used to diagnose rotator cuff tears in individuals who are not able to have MRI scans.
-
5Treatment
Treatment
Left untreated, throwing injuries in the shoulder can become complicated conditions.
Nonsurgical Treatment
In many cases, the initial treatment for a throwing injury in the shoulder is nonsurgical. Treatment options may include:
Activity modification. Your doctor may first recommend simply changing your daily routine and avoiding activities that cause symptoms.
Ice. Applying icepacks to the shoulder can reduce any swelling.
Anti-inflammatory medication. Drugs like ibuprofen and naproxen can relieve pain and inflammation. They can also be provided in prescription-strength form.
Physical therapy. In order to improve the range of motion in your shoulder and strengthen the muscles that support the joint, your doctor may recommend specific exercises. Physical therapy can focus on muscles and ligament tightness in the back of the shoulder and help to strengthen the structures in the front of the shoulder. This can relieve some stress on any injured structures, such as the labrum or rotator cuff tendon.
Change of position. Throwing mechanics can be evaluated in order to correct body positioning that puts excessive stress on injured shoulder structures. Although a change of position or even a change in sport can eliminate repetitive stresses on the shoulder and provide lasting relief, this is often undesirable, especially in high level athletes.
Cortisone injection— If rest, medications, and physical therapy do not relieve your pain, an injection of a local anesthetic and a cortisone preparation may be helpful. Cortisone is a very effective anti-inflammatory medicine. Injecting it into the bursa beneath the acromion can provide long-term pain relief for tears or other structural damage.

Shoulder Pain and Common Shoulder Problems
-
1houlder Pain and Common Shoulder Problems
houlder Pain and Common Shoulder Problems
What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm — from scratching your back to throwing the perfect pitch.
Mobility has its price, however. It may lead to increasing problems with instability or impingement of the soft tissue or bony structures in your shoulder, resulting in pain. You may feel pain only when you move your shoulder, or all of the time. The pain may be temporary or it may continue and require medical diagnosis and treatment.
This article explains some of the common causes of shoulder pain, as well as some general treatment options. Your doctor can give you more detailed information about your shoulder pain
-
2Anatomy
Anatomy
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. A combination of muscles and tendons keeps your arm bone centered in your shoulder socket. These tissues are called the rotator cuff. They cover the head of your upper arm bone and attach it to your shoulder blade.
-
3Cause
Cause
Most shoulder problems fall into four major categories:
- Tendon inflammation (bursitis or tendinitis) or tendon tear
- Instability
- Arthritis
- Fracture (broken bone)
- Other much less common causes of shoulder pain are tumors, infection, and nerve-related problems.
Bursitis
Bursae are small, fluid-filled sacs that are located in joints throughout the body, including the shoulder. They act as cushions between bones and the overlying soft tissues, and help reduce friction between the gliding muscles and the bone.
Sometimes, excessive use of the shoulder leads to inflammation and swelling of the bursa between the rotator cuff and part of the shoulder blade known as the acromion. The result is a condition known as subacromial bursitis.
Bursitis often occurs in association with rotator cuff tendinitis. The many tissues in the shoulder can become inflamed and painful. Many daily activities, such as combing your hair or getting dressed, may become difficult.
Tendinitis
A tendon is a cord that connects muscle to bone. Most tendinitis is a result of inflammation in the tendon.
Generally, tendinitis is one of two types:
Acute. Excessive ball throwing or other overhead activities during work or sport can lead to acute tendinitis.
Chronic. Degenerative diseases like arthritis or repetitive wear and tear due to age, can lead to chronic tendinitis.
The most commonly affected tendons in the shoulder are the four rotator cuff tendons and one of the biceps tendons. The rotator cuff is made up of four small muscles and their tendons that cover the head of your upper arm bone and keep it in the shoulder socket. Your rotator cuff helps provide shoulder motion and stability.Tendon Tears
Splitting and tearing of tendons may result from acute injury or degenerative changes in the tendons due to advancing age, long-term overuse and wear and tear, or a sudden injury. These tears may be partial or may completely separate the tendon from its attachment to bone. In most cases of complete tears, the tendon is pulled away from its attachment to the bone. Rotator cuff and biceps tendon injuries are among the most common of these injuries.
Impingement
Shoulder impingement occurs when the top of the shoulder blade (acromion) puts pressure on the underlying soft tissues when the arm is lifted away from the body. As the arm is lifted, the acromion rubs, or «impinges» on, the rotator cuff tendons and bursa. This can lead to bursitis and tendinitis, causing pain and limiting movement.
Instability
Shoulder instability occurs when the head of the upper arm bone is forced out of the shoulder socket. This can happen as a result of a sudden injury or from overuse.
Shoulder dislocations can be partial, with the ball of the upper arm coming just partially out of the socket. This is called a subluxation. A complete dislocation means the ball comes all the way out of the socket.
Once the ligaments, tendons, and muscles around the shoulder become loose or torn, dislocations can occur repeatedly. Recurring dislocations, which may be partial or complete, cause pain and unsteadiness when you raise your arm or move it away from your body. Repeated episodes of subluxations or dislocations lead to an increased risk of developing arthritis in the joint.
Arthritis
Shoulder pain can also result from arthritis. There are many types of arthritis. The most common type of arthritis in the shoulder is osteoarthritis, also known as «wear and tear» arthritis. Symptoms such as swelling, pain, and stiffness, typically begin during middle age. Osteoarthritis develops slowly and the pain it causes worsens over time.
Osteoarthritis, may be related to sports or work injuries or chronic wear and tear. Other types of arthritis can be related to rotator cuff tears, infection, or an inflammation of the joint lining.
Often people will avoid shoulder movements in an attempt to lessen arthritis pain. This sometimes leads to a tightening or stiffening of the soft tissue parts of the joint, resulting in a painful restriction of motion.
Fracture
Fractures are broken bones. Shoulder fractures commonly involve the clavicle (collarbone), humerus (upper arm bone), and scapula (shoulder blade).
Shoulder fractures in older patients are often the result of a fall from standing height. In younger patients, shoulder fractures are often caused by a high energy injury, such as a motor vehicle accident or contact sports injury.
Fractures often cause severe pain, swelling, and bruising about the shoulder.

Shoulder Separation
-
Shoulder Separation
Shoulder Separation
A shoulder separation is not truly an injury to the shoulder joint. The injury actually involves the acromioclavicular joint (also called the AC joint). The AC joint is where the collarbone (clavicle) meets the highest point of the shoulder blade (acromion).
-
Cause
Cause
The most common cause for a separation of the AC joint is from a fall directly onto the shoulder. The fall injures the ligaments that surround and stabilize the AC joint.
If the force is severe enough, the ligaments attaching to the underside of the clavicle are torn. This causes the separation of the collarbone and the shoulder blade. The shoulder blade (scapula) actually moves downward from the weight of the arm. This creates a bump or bulge above the shoulder.
The injury can range from a mild sprain without a bump to a complete disruption with a very large bump. Good pain-free function often returns even with a very large bump. The greater the deformity, the longer it takes for pain-free function to return.
A mild shoulder separation involves a sprain of the AC ligament that does not move the collarbone and looks normal on X-rays.
A more serious injury tears the AC ligament and sprains or slightly tears the coracoclavicular (CC) ligament, putting the collarbone out of alignment to some extent with a smaller bump.
The most severe shoulder separation completely tears both the AC and CC ligaments and puts the AC joint noticeably out of position, with a larger bump. -
Doctor Examination
Doctor Examination
The injury is easy to identify when it causes deformity. When there is less deformity, the location of pain and x-rays help the doctor make the diagnosis. Sometimes having the patient hold a weight in the hand can increase the deformity, which makes the injury more obvious on x-rays.
-
Treatment
Treatment
Nonsurgical Treatment
Nonsurgical treatments, such as a sling, cold packs, and medications can often help manage the pain. Rarely, a doctor may use more complicated supports to help lessen AC joint motion and pain.
Most people return to near full function with this injury, even if there is a persistent, significant deformity/bump. Some people have continued pain in the area of the AC joint, even with only a mild deformity. This may be due to:
Abnormal contact between the bone ends when the joint is in motion
Development of arthritis
Injury to a disk-like piece of cushioning cartilage that is often found between the bone ends of this joint
It is often worthwhile to wait and see if reasonable function returns without surgical treatment. Most patients, even with very severe injuries, are often managed effectively without surgery.Surgical Treatment
Surgery can be considered if pain persists or the deformity is severe. A surgeon might recommend trimming back the end of the collarbone so that it does not rub against the shoulder blade bone (acromion).
Where there is significant deformity, reconstructing the ligaments that attach to the underside of the collarbone is helpful. This type of surgery works well even if it is done long after the problem started. These operations can be done arthroscopically or open, with a plate or without. Sometimes, if a plate is used to assist with the surgery, it is usually removed after healing of the shoulder separation.
Whether treated conservatively or with surgery, the shoulder will require rehabilitation to restore and rebuild motion, strength, and flexibility.
